AUCTORES
Globalize your Research

Case Report | DOI: https://doi.org/10.31579/2690-4861/139
1 Pediatric Allergy & Immunology, Research Centre of King Saud Medical City, Kingdom of Saudi Arabia.
2 Pediatric Immunology & Allergy, Research Centre of King Saud Medical City, Kingdom of Saudi Arabia.
3 Gen Pediatrics, Research Centre of King Saud Medical City, Kingdom of Saudi Arabia.
4 Pediatrics ID department, Research Centre of King Saud Medical City, Kingdom of Saudi Arabia.
5 Laboratory of Human Genetics of Infectious Diseases, Necker Branch, Institut National de la Santé et de la Recherche Médicale, U980, and University Paris Descartes, Necker Medical School, 75015 Paris, France.
*Corresponding Author: Emadia Alaki, Pediatric Allergy & Immunology, Research Centre of King Saud Medical City, Kingdom of Saudi Arabia.
Citation: E Alaki, Abdulwahab Al Ayoubi, G Alghannam, Abdul-A Alsayegh, A Siddiqi, et al. (2021) A Case Report on Disseminated Candida Lusitaniae Infection And Tuberculous Lymphadenitis in Patient with Compound Heterozygous Pair of Mutations of CYBA Chronic Granulomatous Disease. International Journal of Clinical Case Reports and Reviews. 7(3); DOI: 10.31579/2690-4861/139
Copyright: © 2021 Emadia Alaki, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 25 May 2021 | Accepted: 15 June 2021 | Published: 21 June 2021
Keywords: cgd; cyba; disseminated candida lusitaniae; bcgitis
Chronic granulomatous disease (CGD) is an unusual hereditary chief immune- deficiency disease, which is characterized by nicotinamide adenine dinucleotide phosphate oxidase (NADPH) system malfunction. In this type of disease the phagocytic cells could not be able to destroy the pathogens at the time of development of an infection. This will result in patient's susceptibility to recurrent and intractable microbial infections. The disease is considered to be a genetically heterogeneous having equal susceptibility among all the ethnic groups. Patients with (CGD) suffer from persistent, fatal fungal and bacterial infections of the skin, the lymph nodes, airways, brain, liver, and bones. Whenever there is an infection with any odd microorganisms the susceptibility for CGD rises.
In our article we aim to report a case study of a 4 months old female with disseminated candidiasis Tuberculosis lymphadenitis in details. The infant was treated successfully with antifungal voriconazole and broad spectrum antibacterial agents as well as anti-mycobacterial medications. When the patient was followed up later, it showed regression of the abnormal reports. But later developed CNS Candida and disseminated tuberculous with sequalae. Diagnosis was confirmed as heterozygous CYBA for p22phox, defect by genetic analysis. P22phox is an omnipresent protein which is coded by the gene CYBA located on the long arm of chromosome16. P22phox it is crucial factor of the enzyme superoxide-generating (NADPH) oxidase.
Infection with bacteria, Candida lusitaniae is maximum among the patients who are suffering with haematological malignancies. The chance of the infection rises when the patient is receiving chemotherapy. This type of infection usually occurs among the patients who are presenting fungal infection that has already spread throughout the blood and among them only 7.3% of the patients are showing the symptomatic manifestations of peritonitis. However, the most difficult point is that the laboratory culture is not the answer for the growth of the particular microorganisms as these organisms are extremely difficult to culture or separate.
Chronic granulomatous disease (CGD) is considered to be a disease that can be inherited and it occurs due to the disorder of the superoxide-generating phagocyte NADPH oxidase system. 1 That is the reason why patients who are suffering from the CGD are much more prone to infection caused by catalase positive bacteria and also fungus such as Burkholderia cepacia, Aspergillus, Nocardia sp., Serratia marcescens, and Staphylococcus aureus. Moreover, it is also well known that CGD patients are also more susceptible to infectivity caused by sentinel micro-organisms along with heightened risk for pyogenic microorganisms [1].
Here we are going to present a case study with Chronic granulomatous disease (CGD) showing the symptomatic manifestations of lymphadenitis caused by disseminated Candida lusitaniae and TB(BCG)lymphadenitis. The term disseminated Candida lusitaniae means either the invasive form of candidiasis or immense fungal infection with Candida which surely rapidly spreads up to several visceral organs like kidney, liver, heart, brain, eyes or spleen etc [1, 2]. CGD is also being referred to as “Bridges–Good syndrome”. This is an inherited disease where our lymphatic system cannot produce the Reactive Oxygen Species (ROS). Now CGD is caused mainly due to the mutations observed among one of the five alleles namely CYBA, CYBB, NCF1, NCF2, or NCF4 and these alleles codes for the varied subunits of the enzyme named as NADPH oxidase, which plays a significant responsibility within our immune system [2]. As it is a genetic disorder, therefore it can be observed among the children as it affects the important roles of the certain cells and also to build up immunity against varied germs by our immunity. This particular disorder is treated with antibiotics like antibacterials or the antifungals but it cannot cure the condition [2].
In general, signs and symptomatic manifestations of the CGD are presence of fever, pain in the chest while inhalation or exhalation, inflamed and sore lymph glands, irritation of the skin and the constant running of the nose, rash or swollen redness in the mouth or in the skin [2]. As the infections are associated with the formation of the “granuloma” therefore, the name CGD, however, only a handful of microorganisms cause “granulomas” [3]. Among the bacteria, Mycobacteria, i.e., that causing tuberculosis and also fungi causes formations of granulomas throughout the world [2, 3].
The assays that actually helps in the diagnosis of the granulomas are the neutrophil function test (NFT), and the genetic test that identifies the particular mutations, and dihydrorhodamine reduction assay. The NFT determines that how efficiently the white blood corpuscles (WBC) are tasking throughout our body [3].
The genes of the five NADPH oxidase components are CYBB (located on the X chromosome) encoding gp91phox, and the autosomal genes CYBA encoding p22phox, NCF2 encoding p67phox NCF1 encoding p47phox and NCF4 encoding p40phox. Moreover, 70% of the CGD patients reveal mutation within the CYBB gene (among them mostly are hemizygous males, whereas few are heterozygous females with distorted expression of their mutation).2 mutations in the CYBA gene that encodes for p22phox and also mutations in NCF2 gene, are considered to be very unusual and as per the past scientific evidence about 6% of total CGD cases identified throughout the globe) and lead to AR220CGD. 3 The protein p22phox is expressed from CYBA gene that is present upon chromosome 16q24. Any of these mutant genes can result in the development of CGD. [4]
Patient was a 4-month-old female a product of full-term gestation. She was previously well. She was admitted with history of progressive abdominal distension and fever for the last 2 weeks, no other complains. Patient received BCG vaccine however there are positive family history of TB. No index case of primary immunodeficiency or early death, no consanguinity. Looks sick mild distress, not pale not jaundice, no dysmorphic feature, severe abdominal distension, with generalized tenderness and dilated veins with umbilical hernia, no organomegaly the rest of examinations within normal. All septic, Radiological and Immunological work were done.
Ultrasound test was done and it showed, diffuse increased echogenicity of the visualized bowel loops associated with mild bowel wall thickening and hyperaemia, findings are worrisome for enterocolitis for high clinical concern. Mild to moderate free fluid was noted in the abdomen associated with internal septations predominantly in the sub hepatic region, highly worrisome for superimposed infection /early fluid collection.
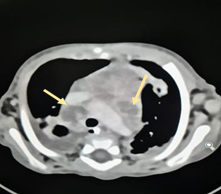
CT scan for Chest, Abdomen, and Pelvis (Figure 1) The impression multiple mediastina, hilar and axillary lymph nodes noted some of them showing central necrosis. Tree in bud airspace opacities, hilar opacities associated with bilateral mild pleural effusion were also noted. Extensive innumerable variable size diffuse scattered abdominal necrotic lymph nodes were noted in a background of severe mesenteric fat stranding, mild ascites with no drainable collection was reported. Differentials may include TB infection, other granulomatous infection; less likely Differentials may include underlying malignancy. After 6 weeks ultrasound repeated show, there are remarkable improvements.
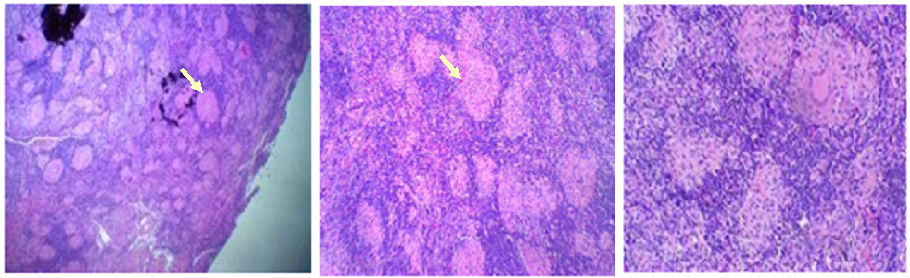
After 4 weeks from admission left an axillary lymph-node biopsy showed: chronic non necrotizing granulomatous lymphadenitis. Refer Figure: 2 Culture for positive AFB, Ziehl- Neelsen stain positive for Acid Fast Bacilli consistent with tubercular lymphadenitis, Negative Grocott methylamine silver (GMS) stain for fungal identification (Refer Figure 3).

She was started on antibiotics amikacin, rifampicin, ethambutol, isoniazid, pyridoxine, methylprednisolone was added. Soon after the start of the antibiotics, patient gradually improved [4]. Follow up of abdominal US showed minimal free fluid noted in the pelvis region. Her medications were later switched to oral, and Amikacin was discontinued and levofloxacin was added. She was having on/off vomiting after feeding, so she was started on omeprazole as well she was discharged on anti-mycobacterial medications.
One month later, patient readmitted with lethargy decreased feeding with vomiting and dehydration and had left facial palsy, hemiplegia. During admission, she developed seizures; she was seen by neurosurgery team and an External Ventricular Drain (EVD) inserted, initial cerebrospinal fluid (CSF) Gram stain and bacterial culture were negative, and polymerase chain reaction (PCR) for mycobacterial tuberculosis also negative [5]. Three weeks later she developed EVD related Candida Lusitania infection where EVD was changed and started on Voriconazole since the patient’s culture report reported the same Candida from urine and abdominal paracentesis.
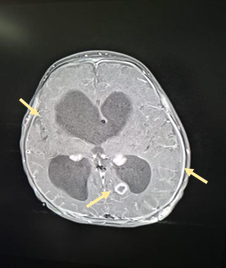
She was initially on Keppra, phenobarbitone and lorazepam, still had breakthrough seizures, lorazepam was changed to Diazepam, and seizures were controlled [5]. CT brain was done initially showing showed hyperdense small shadow in the left periventricular posterior occipital horn medially, called tuberculosis granuloma (Figure 4).

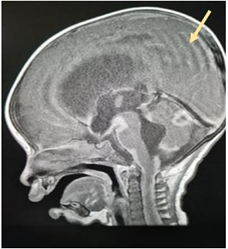
Followed by (MRI) brain &spine showed diffuse infective process involving both cerebral hemisphere with two pockets of abscess in addition to the diffuse thick meningeal enhancement in addition to the moderate communicating hydrocephalus seen supra or infratentorial most like representing infective process as diffuse meningitis representing a picture of central nervous system (CNS) tuberculosis and communicating hydrocephalus, spine show upper cervical disseminated infective process TB vs. pyogenic infection ( Figure 5, 6, 7).

Neurosurgeons were consulted, External Ventricular Drain(EVD) was inserted and the CSF culture grew Candida Lusitaniae with the following sensitivity pattern (sensitive to voriconazole and caspofungin but resistant to fluconazole and Amphotericin B). Patient was kept on Voriconazole for 6 weeks were the patient showed clinical improvement repeated CSF study parameters normalized and culture showed no growth [5]. The previous MRI brain imaging findings was resolved, so Ventricular Peritoneal shunt (VP) was inserted. Patient showed slowly progressive improvement from ascites, and complete resolution of all her symptoms. Due to recurrent ascites which it was believed to be due to VP shunt, patient underwent VP Shunt removal and VA insertion. After the surgery she developed persistent vomiting and lethargy and she went to PICU. She developed seizures, was started lorazepam was changed to Diazepam, seizures were controlled for a while then again break through seizures so Keppra dose increased and Topamax added and weaning phenobarbitone started [5]. As because of the patient’s persistent ascites, ascitic paracentesis were done frequently. The patient became lethargic had abdominal distension and vomiting, looks dehydrated. She was seen by neurosurgeon and the impression shunt failure revealed by CT scan showed communicating hydrocephalus with right subdural collection. Soon after choroid plexuses cauterization and endoscopic 3rd ventricular cystostomy with EVD done and admitted for two days in PICU. Once the patient become more stable, reassess by neurosurgeon VP inserted and observed for any sign of high IC or ascites. Patient clinical stable and discharge in good condition.
Total White Blood Cell (WBC): 20.08 (10^9/L); neutrophils 59.2 %; lymphocytes 33%; haemoglobin is 9.3 g/dl (MCV: 80.9 MCH: 24.3 RDW: 17.6) and the platelet count is 818 (10^9/L). The biochemical report of the patient also showed that the level of urea: is 1.31 mmol/L, creatinine is 25.5 umol/L, serum albumin is 22.9 g/L, lactic acid is 2.05 mmol/L, aspartate amino-transferase (AST) is 43.22 U/L, alanine amino-transferase (ALT) level is 39.95 U/L, and the C-reactive protein (CRP) is 127 mg/L. he following leucocyte markers were reported as follows: T Lymph (CD3+): 46.74%, CD3 Abs Count: 1616.38, B Lymph (CD19+): 32.64%, CD19 Abs Count: 1128.99, NK-lymph (CD1656 Abs Count: 19.35%, CD16+CD56 Abs Count: 669.13, CD3+CD4 Abs Count: 962.39, T suppressor (CD3+CD8+): 18.95%, CD3+CD4 Abs Count: 655.36, T Helper (CD3+CD4+): 27.83%, T Helper, T Suppressor ratio: 1.47%.
Neutrophil oxidative burst test showed reduced in activity.
Influenza A Virus, Corona Virus, Para-influenza Virus, Respiratory Syncytial Virus A/B, Human Metapneumo virus A/B, Adenovirus, Boca virus, Rhinovirus / Enterovirus, Mycoplasma pneumoniae, Legionella pneumophila, Bordetella pertussis were conducted.
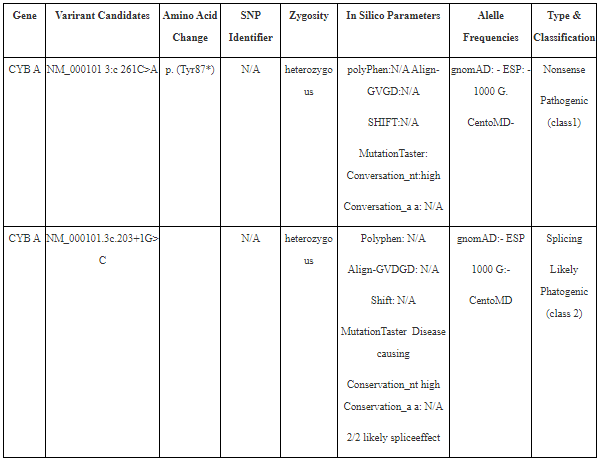
A heterozygous likely pathogenic variant was identified in the CYBA gene. Also, a heterozygous pathogenic variant was identified in the CYBA gene. This like consistent with a genetic diagnosis of Autosomal receive chronic granulomatous disease type 4. Parental carrier testing is needed to identify the phase of the detective variants.
DISCUSSION:
In the case report, it was hypothesized patient suffered from CGD the case is supported by both laboratory and radiological findings.
We had sent sample for the mother, to the Laboratory of Human Genetics of Infectious Diseases, France. DNA extraction was carried out of whole blood by the desired protocol.
This variant has previously been described as disease causing for chronic granulomatous disease heterozygous pair of mutations of CYBA where many of the previous were homozygous [5, 6]. In several cases, the heterozygous parents are observed with respect to the mutations that indicate consanguinity within the family [7-11]. Depending on the prevalence of CGD throughout the globe it is 1 out of 200,000–250,000 live births. The real incidence may be even higher than the predicted incidence, in countries with a higher consanguinity rate, such as Saudi Arabia, Oman and Medial East in general. Therefore, we can find more cases of AR CGD [16].
Mutation analysis of CYBA revealed 12 different mutations, including three novel mutations of CYBA gene in four of 22 Iranian patients with AR‐CGD were found [25]. Other study for genetic analysis show in 32 patients with CGD, 4 (17.4%) carried CYBA variants, and 3 (13%) carried NCF2 variants [26]. In Upper Egypt it was observed that many of the usual mutations are within the CYBA gene [27]. In India cohort study, 41 different mutations were observed where 9 novel mutations were found within the CYBB gene and 2 novel mutations each in the CYBA, NCF1, and NCF2 genes. CGD cases frequently manifested severe and deep- seated infections of the lung, liver skin, brain, and lymph nodes [22, 23]. The majority of infections in CGD are due: S. aureus, Burkholderia cepacia complex, Serratia marcescens, Nocardia species, Aspergillus species, Salmonella, Candida Lusitaniae, Bacille Calmette Guerin (BCG) and tuberculosis are also important [23,24]. As the disease is considered to be a primary immune disorder, it affects our WBC of immune system, such as the neutrophils, monocytes and eosinophils and the macrophages [30]. As mentioned earlier the patient is unable to resist the infections caused by certain specific bacteria and thereafter it develops a chronic infectious and inflammatory disorder [30]. The disorder can affect many parts of the body such as lungs, skin and the bones and other inflamed tissues which are actually very sparsely distributed throughout the parts of the body. The symptomatic manifestations of this particular disorder generally start at the stage of the infancy, however those children who have mild form of this disease will not develop the signs and symptoms till childhood or teenage [30]. The major mechanism of action behind the disease that it fails to produce an enzyme or produces faulty enzyme that could help in the process of killing of microorganisms by the white blood cells (WBCs) [30]. According to the prevalence of this particular disorder, the disease affects the male counterparts more often than the female gender [31]. According to the study of the North America and Europe the disease has affected approximately two third of the individuals who are suffering from the X linked recessive form of the disorder. Therefore, it is also estimated that out of a million about 4 to 5 children are suffering from the CGD [31]. Infection of VP shunts varies between 2 to 27% [12, 13]. Similar cases C. lusitaniae isolated from lymph node [14]. C. lusitaniae which was isolated previously were observed to be resistant to antibiotic amphotericin B [15]. Many CGD patients exhibits regional lymphadenopathy after the BCG vaccination (BCGitis), while the case of disseminated disease (BCGosis) is less frequent [17]. However, study in Saudi Arabia estimated a rate from 0.1 to 4.3 per one million in vaccinated children [18].
As per previous scientific data, 50-76 % of BCG-infected patients mostly shows the symptomatic manifestation of immunodeficiency [19, 20]. CGD, severe combined immunodeficiency disease (SCID), Mendelian susceptibility to mycobacterial disease (MSMD) and hyper-IgM syndrome are the most common PIDs linked with unpleasant events after the vaccination [21].
Since the risk of fatality is more among CGD of all varieties, therefore identification of mutations is necessary for the diagnosis and genetic counseling especially in our country with high consanguinity prevalence 57.7%. 29 CGD treatment usually includes various modalities of treatments, and prophylactic antifungals and antibiotics. Prophylactic recombinant human interferon-γ, immunosuppresses or immune modulators may be, supportive. However, hematopoietic stem cell transplantation and gene therapy are recently developed options for the treatment cure of CGD [29].
Thus, CGD patients receive the prophylaxis for the antibacterial and the antifungal. In general, the antibiotic that is prescribed to the patient of CGD is the trimethoprim- sulfamethoxazole, and it is generally given for the antibacterial infections. Past data have revealed that this particular antibiotic is generally given to the patients of the CGD as they have the activity against the majority of the antibacterial infections.
The pathological condition of the CGD have revealed that the condition may often include the following areas of the physiological system such as pneumonias, liver abscesses, skin infections such as skin abscesses, lymphadenitis and osteomyelitis. Moreover, it should be noted that there is a high proneness to CGD, when infections occur with Candida lusitaniae, and Mycobacterim tuberculosis and these organisms are not considered to be sentinel organism for the diseased condition of CGD. However, this also proved that new-borns should be potentially screened for the CGD.
Conclusion:
Chronic granulomatous disease (CGD) is a disorder which is inheritable and this actually happens due to disorder of the superoxide-generating phagocyte NADPH oxidase system. In this paper a case study has been detailed of a 4 months old female case patient with all the related laboratory and radiological findings. From the past scientific literatures, it has been confirmed that infection with bacteria, Candida lusitaniae is maximum among the patients who are suffering with haematological malignancies. Moreover, the disease is considered to be a genetically heterogeneous having equal susceptibility among all the ethnic groups. It has been observed that whenever there is an infection with any rare microorganisms the susceptibility for the disease rises.
Clearly Auctoresonline and particularly Psychology and Mental Health Care Journal is dedicated to improving health care services for individuals and populations. The editorial boards' ability to efficiently recognize and share the global importance of health literacy with a variety of stakeholders. Auctoresonline publishing platform can be used to facilitate of optimal client-based services and should be added to health care professionals' repertoire of evidence-based health care resources.

Journal of Clinical Cardiology and Cardiovascular Intervention The submission and review process was adequate. However I think that the publication total value should have been enlightened in early fases. Thank you for all.

Journal of Women Health Care and Issues By the present mail, I want to say thank to you and tour colleagues for facilitating my published article. Specially thank you for the peer review process, support from the editorial office. I appreciate positively the quality of your journal.

Journal of Clinical Research and Reports I would be very delighted to submit my testimonial regarding the reviewer board and the editorial office. The reviewer board were accurate and helpful regarding any modifications for my manuscript. And the editorial office were very helpful and supportive in contacting and monitoring with any update and offering help. It was my pleasure to contribute with your promising Journal and I am looking forward for more collaboration.

We would like to thank the Journal of Thoracic Disease and Cardiothoracic Surgery because of the services they provided us for our articles. The peer-review process was done in a very excellent time manner, and the opinions of the reviewers helped us to improve our manuscript further. The editorial office had an outstanding correspondence with us and guided us in many ways. During a hard time of the pandemic that is affecting every one of us tremendously, the editorial office helped us make everything easier for publishing scientific work. Hope for a more scientific relationship with your Journal.

The peer-review process which consisted high quality queries on the paper. I did answer six reviewers’ questions and comments before the paper was accepted. The support from the editorial office is excellent.

Journal of Neuroscience and Neurological Surgery. I had the experience of publishing a research article recently. The whole process was simple from submission to publication. The reviewers made specific and valuable recommendations and corrections that improved the quality of my publication. I strongly recommend this Journal.

Dr. Katarzyna Byczkowska My testimonial covering: "The peer review process is quick and effective. The support from the editorial office is very professional and friendly. Quality of the Clinical Cardiology and Cardiovascular Interventions is scientific and publishes ground-breaking research on cardiology that is useful for other professionals in the field.

Thank you most sincerely, with regard to the support you have given in relation to the reviewing process and the processing of my article entitled "Large Cell Neuroendocrine Carcinoma of The Prostate Gland: A Review and Update" for publication in your esteemed Journal, Journal of Cancer Research and Cellular Therapeutics". The editorial team has been very supportive.

Testimony of Journal of Clinical Otorhinolaryngology: work with your Reviews has been a educational and constructive experience. The editorial office were very helpful and supportive. It was a pleasure to contribute to your Journal.

Dr. Bernard Terkimbi Utoo, I am happy to publish my scientific work in Journal of Women Health Care and Issues (JWHCI). The manuscript submission was seamless and peer review process was top notch. I was amazed that 4 reviewers worked on the manuscript which made it a highly technical, standard and excellent quality paper. I appreciate the format and consideration for the APC as well as the speed of publication. It is my pleasure to continue with this scientific relationship with the esteem JWHCI.

This is an acknowledgment for peer reviewers, editorial board of Journal of Clinical Research and Reports. They show a lot of consideration for us as publishers for our research article “Evaluation of the different factors associated with side effects of COVID-19 vaccination on medical students, Mutah university, Al-Karak, Jordan”, in a very professional and easy way. This journal is one of outstanding medical journal.

Dear Hao Jiang, to Journal of Nutrition and Food Processing We greatly appreciate the efficient, professional and rapid processing of our paper by your team. If there is anything else we should do, please do not hesitate to let us know. On behalf of my co-authors, we would like to express our great appreciation to editor and reviewers.

As an author who has recently published in the journal "Brain and Neurological Disorders". I am delighted to provide a testimonial on the peer review process, editorial office support, and the overall quality of the journal. The peer review process at Brain and Neurological Disorders is rigorous and meticulous, ensuring that only high-quality, evidence-based research is published. The reviewers are experts in their fields, and their comments and suggestions were constructive and helped improve the quality of my manuscript. The review process was timely and efficient, with clear communication from the editorial office at each stage. The support from the editorial office was exceptional throughout the entire process. The editorial staff was responsive, professional, and always willing to help. They provided valuable guidance on formatting, structure, and ethical considerations, making the submission process seamless. Moreover, they kept me informed about the status of my manuscript and provided timely updates, which made the process less stressful. The journal Brain and Neurological Disorders is of the highest quality, with a strong focus on publishing cutting-edge research in the field of neurology. The articles published in this journal are well-researched, rigorously peer-reviewed, and written by experts in the field. The journal maintains high standards, ensuring that readers are provided with the most up-to-date and reliable information on brain and neurological disorders. In conclusion, I had a wonderful experience publishing in Brain and Neurological Disorders. The peer review process was thorough, the editorial office provided exceptional support, and the journal's quality is second to none. I would highly recommend this journal to any researcher working in the field of neurology and brain disorders.
Dear Agrippa Hilda, Journal of Neuroscience and Neurological Surgery, Editorial Coordinator, I trust this message finds you well. I want to extend my appreciation for considering my article for publication in your esteemed journal. I am pleased to provide a testimonial regarding the peer review process and the support received from your editorial office. The peer review process for my paper was carried out in a highly professional and thorough manner. The feedback and comments provided by the authors were constructive and very useful in improving the quality of the manuscript. This rigorous assessment process undoubtedly contributes to the high standards maintained by your journal.

International Journal of Clinical Case Reports and Reviews. I strongly recommend to consider submitting your work to this high-quality journal. The support and availability of the Editorial staff is outstanding and the review process was both efficient and rigorous.

Thank you very much for publishing my Research Article titled “Comparing Treatment Outcome Of Allergic Rhinitis Patients After Using Fluticasone Nasal Spray And Nasal Douching" in the Journal of Clinical Otorhinolaryngology. As Medical Professionals we are immensely benefited from study of various informative Articles and Papers published in this high quality Journal. I look forward to enriching my knowledge by regular study of the Journal and contribute my future work in the field of ENT through the Journal for use by the medical fraternity. The support from the Editorial office was excellent and very prompt. I also welcome the comments received from the readers of my Research Article.

Dear Erica Kelsey, Editorial Coordinator of Cancer Research and Cellular Therapeutics Our team is very satisfied with the processing of our paper by your journal. That was fast, efficient, rigorous, but without unnecessary complications. We appreciated the very short time between the submission of the paper and its publication on line on your site.

I am very glad to say that the peer review process is very successful and fast and support from the Editorial Office. Therefore, I would like to continue our scientific relationship for a long time. And I especially thank you for your kindly attention towards my article. Have a good day!

"We recently published an article entitled “Influence of beta-Cyclodextrins upon the Degradation of Carbofuran Derivatives under Alkaline Conditions" in the Journal of “Pesticides and Biofertilizers” to show that the cyclodextrins protect the carbamates increasing their half-life time in the presence of basic conditions This will be very helpful to understand carbofuran behaviour in the analytical, agro-environmental and food areas. We greatly appreciated the interaction with the editor and the editorial team; we were particularly well accompanied during the course of the revision process, since all various steps towards publication were short and without delay".

I would like to express my gratitude towards you process of article review and submission. I found this to be very fair and expedient. Your follow up has been excellent. I have many publications in national and international journal and your process has been one of the best so far. Keep up the great work.

We are grateful for this opportunity to provide a glowing recommendation to the Journal of Psychiatry and Psychotherapy. We found that the editorial team were very supportive, helpful, kept us abreast of timelines and over all very professional in nature. The peer review process was rigorous, efficient and constructive that really enhanced our article submission. The experience with this journal remains one of our best ever and we look forward to providing future submissions in the near future.

I am very pleased to serve as EBM of the journal, I hope many years of my experience in stem cells can help the journal from one way or another. As we know, stem cells hold great potential for regenerative medicine, which are mostly used to promote the repair response of diseased, dysfunctional or injured tissue using stem cells or their derivatives. I think Stem Cell Research and Therapeutics International is a great platform to publish and share the understanding towards the biology and translational or clinical application of stem cells.

I would like to give my testimony in the support I have got by the peer review process and to support the editorial office where they were of asset to support young author like me to be encouraged to publish their work in your respected journal and globalize and share knowledge across the globe. I really give my great gratitude to your journal and the peer review including the editorial office.

I am delighted to publish our manuscript entitled "A Perspective on Cocaine Induced Stroke - Its Mechanisms and Management" in the Journal of Neuroscience and Neurological Surgery. The peer review process, support from the editorial office, and quality of the journal are excellent. The manuscripts published are of high quality and of excellent scientific value. I recommend this journal very much to colleagues.

Dr.Tania Muñoz, My experience as researcher and author of a review article in The Journal Clinical Cardiology and Interventions has been very enriching and stimulating. The editorial team is excellent, performs its work with absolute responsibility and delivery. They are proactive, dynamic and receptive to all proposals. Supporting at all times the vast universe of authors who choose them as an option for publication. The team of review specialists, members of the editorial board, are brilliant professionals, with remarkable performance in medical research and scientific methodology. Together they form a frontline team that consolidates the JCCI as a magnificent option for the publication and review of high-level medical articles and broad collective interest. I am honored to be able to share my review article and open to receive all your comments.

“The peer review process of JPMHC is quick and effective. Authors are benefited by good and professional reviewers with huge experience in the field of psychology and mental health. The support from the editorial office is very professional. People to contact to are friendly and happy to help and assist any query authors might have. Quality of the Journal is scientific and publishes ground-breaking research on mental health that is useful for other professionals in the field”.

Dear editorial department: On behalf of our team, I hereby certify the reliability and superiority of the International Journal of Clinical Case Reports and Reviews in the peer review process, editorial support, and journal quality. Firstly, the peer review process of the International Journal of Clinical Case Reports and Reviews is rigorous, fair, transparent, fast, and of high quality. The editorial department invites experts from relevant fields as anonymous reviewers to review all submitted manuscripts. These experts have rich academic backgrounds and experience, and can accurately evaluate the academic quality, originality, and suitability of manuscripts. The editorial department is committed to ensuring the rigor of the peer review process, while also making every effort to ensure a fast review cycle to meet the needs of authors and the academic community. Secondly, the editorial team of the International Journal of Clinical Case Reports and Reviews is composed of a group of senior scholars and professionals with rich experience and professional knowledge in related fields. The editorial department is committed to assisting authors in improving their manuscripts, ensuring their academic accuracy, clarity, and completeness. Editors actively collaborate with authors, providing useful suggestions and feedback to promote the improvement and development of the manuscript. We believe that the support of the editorial department is one of the key factors in ensuring the quality of the journal. Finally, the International Journal of Clinical Case Reports and Reviews is renowned for its high- quality articles and strict academic standards. The editorial department is committed to publishing innovative and academically valuable research results to promote the development and progress of related fields. The International Journal of Clinical Case Reports and Reviews is reasonably priced and ensures excellent service and quality ratio, allowing authors to obtain high-level academic publishing opportunities in an affordable manner. I hereby solemnly declare that the International Journal of Clinical Case Reports and Reviews has a high level of credibility and superiority in terms of peer review process, editorial support, reasonable fees, and journal quality. Sincerely, Rui Tao.

Clinical Cardiology and Cardiovascular Interventions I testity the covering of the peer review process, support from the editorial office, and quality of the journal.
